A common complaint amongst patient’s who have been prescribed foot orthotics is ‘pain in the arch’. This type of pain can be the result of 4 common issues:
1) Pain can be due calcification (similar to dupuytren’s contracture) or a fibroma in the body of the Plantar Fascia, or a Ganglion cyst may be present. Dupuytren’s contracture in the fascia of the foot is called Ledderhose disease, or plantar fascial fibromatosis, and is sometimes associated with plantar fasciitis.
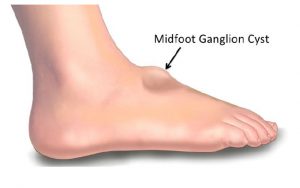
A ganglion cyst is a tumor or swelling on top of a joint or the covering of a tendon (tissue that connects muscle to bone). Ganglion cysts are among the most common benign soft-tissue masses. Although they most often occur on the wrist, they also frequently develop on the foot usually on the top, but can also occur on the plantar surface. Ganglion cysts vary in size, may get smaller and larger and may even disappear completely, only to return at another time. The exact cause of ganglion cysts is un-known, they may arise from trauma whether a single event or repetitive microtrauma.
TREATMENT: If there is calcification in the fascia, use manual therapy to break it down. For a fibroma or Ganglion cyst, a deflection will need to be heated into the orthotic using a deflective device such as a spoon, to accommodate and relieve any pressure from this area.
2) Plantar fasciitis pain can be experienced at the attachment to the calcaneus. It is also refered to as Plantar Fasciosis a degenerative syndrome of the plantar fascia resulting from repeated trauma at its origin on the calcaneus1.
TREATMENT: Control rearfoot pronation using orthotics with intrinsic rearfoot posting to realign the feet to the Subtalar Joint Neutral Position (STJN).
If additional inversion is required to control and achieve STJN, add extra rearfoot wedges (2° or 4°) to provide additional Calcaneal control2.
A medial arch infill can also be applied to the orthotic to provide increased arch support.
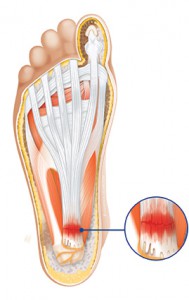
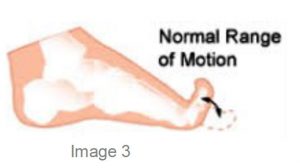
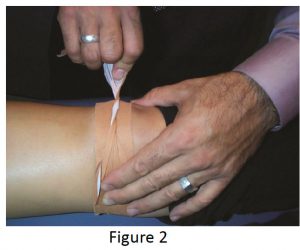
3) The Plantar fascia may be tight, and during gait (at mid stance to toe-off), compressing into the medial longitudinal arch of the orthotic causing discomfort and pain. To test for a tight fascia use the ‘Windlass Test’ (pictured below).
TREATMENT: Create a plantar fascial ‘relief’ or ‘groove’ in the arch of the orthotic using heat or by grinding the orthotic. Place the groove 1 cm from the medial edge through the arch contour. Watch video here.
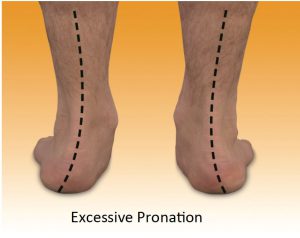
4) The patient may exhibit unilateral excessive pronation as a possible compensation or due to plantar injury.
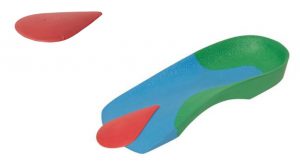
TREATMENT: Unilateral arch pain can be associated with a leg length difference3 due to long leg compensatory excessive pronation. If a structural leg length discrepancy is identified, a heel lift will need to applied to the orthotic on the shorter leg.
SAVE 10% OFF ICB PRODUCTS WITH DISCOUNT CODE: 02ICB10 Offer online only!
The issue of ‘Forefoot Varus’ is an interesting one as there are several misunderstandings in relation to this osseous condition. The first issue is the confusion in relation to Forefoot Varus and Forefoot Supinatus – the former being osseous in nature and the latter a soft tissue condition. The second issue is the proliferation of confusing terminology such as Forefoot Varus, Supinatus, flexible forefoot varus and forefoot invertus, to name a few.
Therefore it can be said that a ‘forefoot varus is a cause of ‘overpronation’ and a forefoot supinatus is the result of ‘overpronation’.1
Merriman’s1 Assessment of the lower limb indicates that:
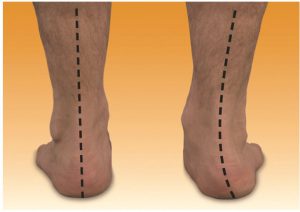
The Varus foot appears supinated with the lateral border of the foot rela-tively plantarflexed in comparison with the Medial border.
An inverted foot may be due to :
True forefoot varus. Boney abnor-mality, theoretically due to inadequate torsion of the head and neck of the talus during fetal development, but this is not well supported (Kidd 1997)
The presence of a true forefoot varus is said to lead to a very flat foot with no longitudinal arch (Grumbine 1987)
Forefoot supinatus is Acquired soft tissue deformation due to abnormal pronation of the rearfoot. The forefoot Is held in an inverted position be-cause of soft tissue contraction.
It can be difficult to differentiate be-tween a Forefoot Varus and a Fore-foot Supinatus.
The most common test is where a plantar grade pressure is applied to the dorsum of the 1st ray or metatarsal. The 1st Metatarsal shaft should plantarflex and is this does not occur then it is deemed to be fixed osseous condition, whereas if it is mobile or there is some ability to move in a plantarflex direction it a Forefoot Supinatus.
In summary ….a forefoot varus differs from forefoot supinatus in that a fore-foot varus is a congenital osseous deformity that induces subtalar joint pronation, whereas forefoot supinatus is acquired and develops because of subtalar joint pronation.2
Other conditions3 that are due to inverted forefoot are:
A) Dorsiflexed 1st Ray( metatar-sus Primus)
B) Plantarflexed 5th ray both fixed and mobile are possible.3
Assessment : The Varus foot often looks banana shaped and the navicular has dropped and is excessively everted.
The supinatus foot mimics the Varus foot in most respects, however, the banana shape is not as prevalent and it is able to be distinguished by the ‘Supinatus – Varus test’.
Orthotic Prescription: Forefoot Varus
When devising the orthotic prescription, firstly the mobility of the rearfoot should be assessed.
If the Rearfoot is mobile, medium to firm orthotics can be prescribed to support and control the foot, with a forefoot varus addition posted to the medial forefoot.
Alternatively, if the rearfoot is mobile and requires additional inversion (i.e more than the intrinsic posting in the orthotic device) an inversion ramp can be attached to the entire medial aspect of the orthotic.
Orthotic with Inversion Ramp.
When the patient has a fixed or arthritic rearfoot, then soft to mid density accommodative orthotics are more effective, with a forefoot varus wedge attached to the medial forefoot. This type of foot can, because of the mobile forefoot, experience conditions such as, Metatarsalgia, morton’s neuroma & mid tarsal periostitis.
Periostitis is an inflammation of the covering of the bones, if left untreated it can progress to a stress fractures.
The Forefoot Varus Addition on the orthotic fills the space under the 1st MTPJ providing the mechanism for toe off to occur by creating normal ground reaction forces to occur at toe off in gait.
Soft orthotic for fixed rearfoot
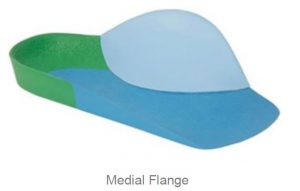
In both cases (i.e. mobile & fixed rearfoot with forefoot varus) extra support can be provided by applying medial flanges (soft or firm) to the dorsal arch area which can also assist in reducing friction on the medial aspect of the foot. Orthotic Prescription: Forefoot Supinatus.
Patient’s exhibiting a forefoot supinatus do not require any additional medial forefoot wedging or modification to the orthotic device .
The reason for this is that once the foot is inside the shoe wear the shoe ‘sock’ upper will assist in a plantarflex action to the dorsum of the foot and this will assist in stretching the contracted soft tissue.
Adding or Posting medial addition or wedge to a SUPINATUS condition will ultimately create a disruption and exostosis between the articulation of the medial cuneiform and base of the first metatarsal at the medial cuneiform joint (1st tarsometatarso joint). .4.
References :
1. Merriman’s Assessment of the lower limb Ed 3 p259-261
The term Pes cavus is derived from Latin meaning ‘hollow foot’ and covers a wide spectrum of foot deformities.
The Pes cavus foot can be hereditary or acquired and the underlying causes can be neurological, orthopaedic or neuromuscular. The condition can be wide ranging from conditions such as Chartcot-marie-tooth disease (CMT) and Fiedreich’s ataxia to the more commonly high arched supinated foot acquired from familial predisposition.
The CMT foot symptoms are progressive and can include :
• Ankle weakness
• High arches
• Clawed toes
• Muscle wasting
• Poor balance
• Muscle weakness in hands and feet
• Peripheral neuropathy
More commonly the condition is not so severe and is generally characterised by an abnormally high medial longitudinal arch, is described as a high axis foot and is most commonly associated with a high forefoot valgus deformity. Other features often include a varus (inverted) calcaneus, a plantarflexed position of the first metatarsal and adducted forefoot together with dorsal contracture of the toes or hammer toes.
Pes cavus feet will invariably be identified as supinated feet and characterised as having ‘reduced or limited pronation’.1 Population-based studies suggest that the prevalence of the cavus foot is approximately 10% 2 .The high arched cavus foot has a decreased range of motion, increased stiffness, and decreased pronatory compensation1.
Often this type of foot will exhibit increased rearfoot varus together with a higher incidence of lateral instability of the foot and ankle1.
Valmassy3 outlines 6 characteristics of a cavus foot:
1) Limited pronation
2) Rigidity
3) Uneven weight distribution
4) Digital contractures (clawing of the toes)
5) Increased tendency to lateral ankle instability with associated ankle sprains
Valmassy3 states that besides the genetic predisposition or familial predisposition other causes to this condition are many and varied such as: Congenital plantarflexed 1st Ray deformity; spasm of peroneus longus; spasm of posterior tibial; weakness of peroneus brevis; weakness of peroneus longus; clubfoot deformity; metatarsus adductus. Underlying causative factors may include but not limited to: Charcot-Marie-Tooth disease, Friedreich’s ataxia, poliomyelitis, spina bifida to name a few.
A study of painful Pes Cavus feet ‘indicates that custom foot orthoses are more effective than a control for reducing cavus foot pain and associated limitation in function.
The key feature of a successful orthotic device for this patient population is a contoured flexible shell moulded to the exact morphology of the foot, with a full-length cushioned top cover. Such a device has the effect of reducing and redistributing abnormal plantar pressure loading. For patients presenting to the clinician with painful cavus feet, custom foot orthoses are an effective treatment option 2.
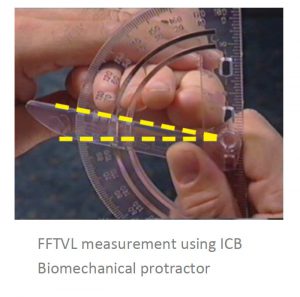
Commonly Pes cavus feet present with Forefoot Valgus deformity (FFTVL) and it is wise in the assessment to complete a FFTVL assessment.
Use a forefoot valgus addition on the orthotic to reduce forefoot instability and lateral inversion of the foot by locking the 4th and 5th columns to mimic ground reaction forces.
High arched feet do not usually require a rigid orthotic support, rather a softer accommodative device such as soft or mid density EVA materials.
However, it is important to mould the orthotic well into the arch and use a metatarsal dome to reposition and lift the transverse arch if the toes are clawing.
REFERENCES
1. Steven Subotnick Sports Medicine of the Lower Extremity Edition 2 p129
2. Joshua Burns, PhD, Jack Crosbie, PhD, Robert Ouvrier, MD, Adrienne Hunt, PhD, Effective Or-thotic Therapy for the Painful Cavus Foot- A Ran-domized Controlled Trial Journal of the American Podiatric Medical Association • Vol 96 • No 3 • May/June 2006
3. VALMASSY, R.L. (1996) Pathomechanics of Lower Extremity Function. Clinical Biomechanics of the Lower Extremity, p. 61, Mosby, St Louis.
Leg length Inequality and the pathogenesis or the origin and development of the condition, is and will always be, a controversial subject. There is a wide variance of opinion on the significance of structural leg length and the various methods for measurement.
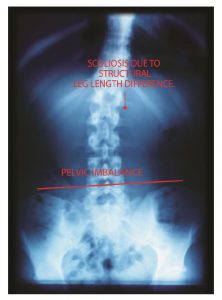
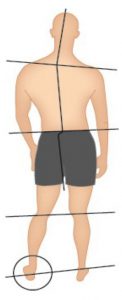
Measuring of structural leg length when treating with orthotic therapy is necessary as undiagnosed structural leg length compensation will be affected when orthotics are prescribed for the patient. The natural body compensations for leg length difference can range from long leg flexion, to short leg supination amongst others as the body seeks to rebalance pelvic alignment. The most common compensation is long leg excessive pronation, accounting for around 80% of the long leg compensations. However in very large structural differences, short leg toe walking and short leg excessive pelvic drop may be taken up as compensations with inevitable upper spine outcomes such as functional scoliosis.
Managing a treatment protocol to assist in minimising issues can be difficult especially if the spine is fixed, that is, the spine (or spinal segment) is not mobile or correctable by conservative means. This is often referred to as a Fixed Sagittal Imbalance (FSI) and conservative treatment looks to make the patient as comfortable as possible when surgical intervention is not undertaken.
In this newsletter we will focus on conservative treatment methods that can be adopted when the osseous structure is mobile.
Assessment for structural leg length difference as part of the initial assessment will avoid removal of undiagnosed compensations and provide an understanding of the size and extent of the leg length difference .
There are many ways to measure leg length, tape measure, x-ray, physical assessment of the limbs such as Palpation for Supine Medial Malleoli Asymmetry Technique 1
ICB provides both 10mm and 15mm extended heel lifts which can be used when the patient has custom made orthopaedic shoes or is wearing boots or the shoe has extra depth in the heel cup as they can be accommodated inside the shoe wear.
The extended heel lift is designed with a longer profile to support the mid foot and eliminate any mid foot collapse which can occur in Heel lift Larger than 8mm high. ICB regular heel lifts are available in S/M/L heel 4/6/8mm and the extended model is available in 10 &15mm.
Generally leather dress shoes can cope with a heel lift up to 6- 8mm (depending upon heel cup height) when added to the orthotic, higher than that the patient may complain that their heel is slipping out of the shoe.
Therefore, alternate shoe styles or modifications need to be considered to accommodate for large structural differences. When recommending shoes with orthotics a deep heel cup is an advantage.
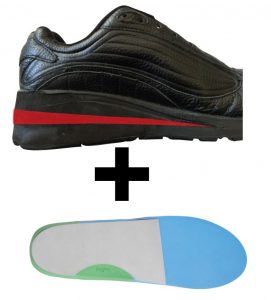
Cross trainers and boots are able to accommodate a larger amount of heel lift in the heel cup, however this may limit the patient to a smaller selection of fashion shoe styles. A solution may be to add maximum amount to the orthotic and then modify the patient’s shoe to achieve the best result. (see below)
To incorporate an intrinsic lift, the sole of the shoe should not contain gel, air cushion pockets and have a base that is flat with no arch cut out. A boot maker can cut the EVA sole with a band saw, finishing behind the breakpoint or 1st MTPJ when the heel lift is less than 30mm. This will enable a normal walking pattern and toe off to occur.
Once the intrinsic heel lift in the shoe sole is over 30mm the cut in the sole must extend to the sulcus behind the phalanges and if a greater amount, to the end of the foot in a thicker ‘ramp’ like adjustment.
The patient featured presented with a condition that could be treated with orthotics , an additional heel lift or raise was recommended to be placed into the heel of the shoe by a boot maker or shoe repairer.
A temporary Heel Lift was used to validate the treatment suggestion note the RIGHT shoe with temporary extrinsic addition which successfully corrected the functional
Extrinsic Heel Lift under shoe heel (above)
scoliosis, this is the amount that should be added into the shoe sole.
Note: It is recommended that both left and right feet are fitted with an orthotic, in addition to any heel lift requirements, to ensure the foundation of the body is balanced.
Generally most footwear will accommodate an orthotic with a 6-8mm heel lift addition (depending upon heel cup height). If a larger heel lift is required(10mm +), extra depth footwear or boots may be required – or alternatively, adjustments to the footwear to incorporate a partial lift into the sole of the footwear can assist.
Reference: 1. Gary Fryer 2005 : Factors affecting the intra-examiner and inter-examiner reliability of palpation for supine medial malleoli asymmetry .
Tibial torsion has been defined as torsion of tibia bone along its longitudinal axis1, which produces a change in alignment of the planes of motion of the proximal and distal articulations, it is a twist in the osseous structure.
This definition draws a distinction between both Tibial Torsion (twist in the bone) and Tibial rotation.
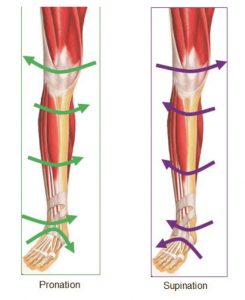
Tibial Rotation occurs when the tibia internally or externally rotates along its axis as a functional outcome of biomechanical forces such as supination and pronation.
Tibial rotation is the rotation of the entire tibial shaft (bone) which takes place in gait as the foot pronates and supinates. The Tibia can exhibit both torsion and rotation and this makes this subject both interesting and somewhat difficult.
Tibial torsion occurs where the tibia exhibits a twist in the actual bone and is apparent from birth.
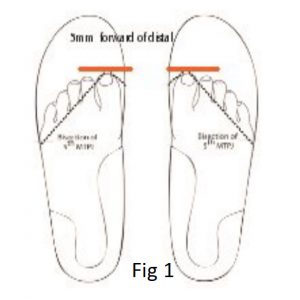
The biomechanical condition can be treated prior to skeletal maturity using foot orthotic devices which work to un torsion the tibia (see Fig 1) .
Once skeletal maturity has occurred, the soft tissue structures are engaged within the body to correct and adjust by tightening and or elongating as the means of correction or repositioning of the foot structure. In both instances knowledge of tibial torsion and tibial rotation will be invaluable to practitioners, in the design and implementation of treatments for their patients.
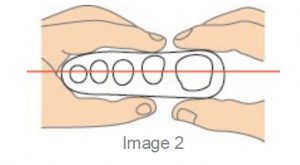
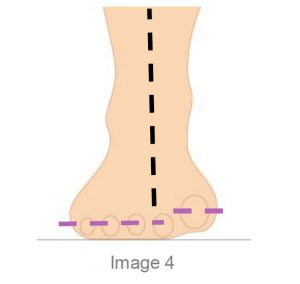
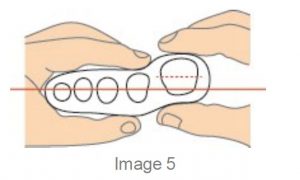
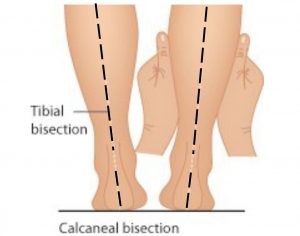
The broad parameters for identifying Tibial torsion have been outlined by Dr Merton Root 2 and Ronald L. Valmassy DPM3 and others, in which it is stated that torsion of the tibia be undertaken by measurement of the position of the medial and lateral malleoli apexes, (see Fig 2) a technique known as the Malleoli Position. (M.P.) This method imagines a pin bisecting medial and lateral malleoli apexes whilst the knee joint is maintained in the neutral position.
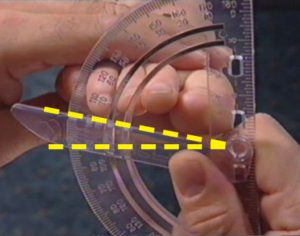
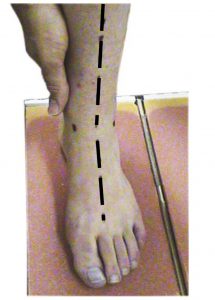
Several tibial torsion measurement techniques have been used or recommended by researchers; radiological methods and arthropometric methods, such as gravity goniometers. The method of measurement generally used in clinical practice is either by eye or by use of a gravity goniometer to measure malleoli positioning. (see Fig 3)
By Eye assessment
Gravity Goniometer
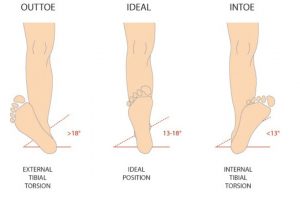
Root and Valmassey reported that the average normal position of the normal malleolar position M.P. was 13° – 18° 2, or slight out toed position.
The malleolar position is determined by observing the bisection of apex of the medial and lateral malleolar whilst the knee joint remained in the neutral position and the patient in the supine position.
Due to the occurrence of displacement of the patella it should be noted that research groups stipulate the position of the knee joint not patella as neutral in the sagittal plane. The positioning of the knee joint was achieved by the using of the knee condyles and lifting in the sagittal plane, ensuring that no lateral or medial deviation is observed.
There are believed to be several causes of the Tibial Torsion condition such as :
a) Acquired: due to injury / trauma such as a broken tibia which is re-positioned and takes on a post-operative internal or external position.
b) Genetics: congenital which is inherited from the mother, father or their genetic lines.
c) Acquired or caused by the environment, especially the uterine environment such as positioning in the womb – the tibia can form in an internal or external torsion position.
When treating in the field of paediatrics it should be noted that Tibial Torsion can effect the gait pattern which, if left untreated may have considerable affect upon the child as it grows to maturity. The outcome may leave the child’s biomechanical structure compromised, leading to other pathologies as the body seeks to compensate for these changes.
Traditionally paediatric biomechanical foot problems were given a low priority, with the result that manageable cases were left untreated and secondary features related to structural pathologies developed. Michaud comments that – ‘Early recognition and management, of actual foot problems in the young would go a long way to the reduction of issues later in life’ 4.
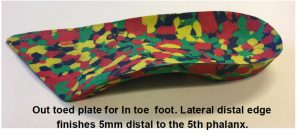
‘Gait plate’ orthotic treatment is a simple and effective method of restoring the lower limb to the ‘normal Malleoli Positioning range of 13° to 18° for children over the age of 6 years.
The gait plate orthotic device is manufactured to provide an extension under the 5th phalange for in-toe or under the hallux for out-toe. In gait the gait plate extension is identified by the proprioception system in the body and the brain instructs the body to reposition the foot in an automated response pattern, gently working on removing the bone torsion in an attempt to reposition to the 13-18° position.
The method is gentle and persuasive and has measurable results , however it appears to be most effective during ‘growth spurts’ in children.
If left untreated the body will naturally attempt to correct by using soft tissues to cosmetically correct the in toed or out toed position. Abnormal foot positioning, i.e. that which is opposed to what is accepted as ‘ideal’ or normal, encourages the body to use soft tissue to en-gage compensatory mechanisms.
Some studies have actually concluded that tight rotators and adductors have a compensatory repositioning function, as in the case of out toe and in toe positioning, relating to tibial torsion. 5,6,7,8, Again it must be stated that this is not strictly the case in every situation, and as such a small number of patients may present with tibial torsion without exhibiting hip compensations. The reasons for a lack of compensatory muscle tightness are unknown. These compensatory mechanisms can move joints in the body outside the normal range of motion and in the pro-cess may lead to so called ‘idiopathic’ soft tissue tight-ness such as Tight Abductors & Adductors or alternatively joint soreness during the compensation process.
References:
1. MULLAJI Arun B, SHARMA Amit K,1 MARAWAR Satyajit V, and KOHLI AF. Tibial Torsion in Non-Arthritic Indian Adults: A Computer Tomography Study of 100 Limbs.
2. ROOT ML, ORIEN WP, WEED JH, HUGHES R, Biomechanical Ex-amination of the Foot The Orthotic Solution I 67 Vol 1. p34, 1971
3. VALMASSY R.L., (1996) Clinical Biomechanics of the Lower Ex-tremeties. p255
4. MICHAUD, T.C (1997): Foot Orthoses and Other Forms of Conserva-tive Foot Care. Sydney: Williams & Wilkins, p168.
5. STAHELI, LT. In-toeing and Out-toeing in Children. Journal Family Practice. May 1983;16(5):1005-11.
6. STAHELI LT, CORBETT M, WYSS C, KING H. Lower Extremity Rota-tional Problems in Children. Normal Values to Guide Management. American Journal Bone Joint Surgery Jan 1985;67(1):39-47.
7.DAVIDS JR, DAVIS RB. Tibial Torsion: Significance and Measure-ment. Gait Posture. Jul 2007;26(2):169-71.
Posterior tibial tendon dysfunction (PTTD) is a condition that results in inflammation or tearing of the posterior tibial tendon.
The Tibialis Posterior is an inverter and plantar flexor of the foot1. The Posterior Tibial Tendon is the major dynamic stabiliser of the foot in pre-venting rearfoot eversion or pronation and is subject to repetitive overuse injury such as, peritendinitis, inflammation of the tendon sheath, and rupture2. Often the early stages of the condition can be overlooked or misdiagnosed3.
PTTD can be experienced bilaterally and or unilaterally, typically beginning with a paratenonitis of the tendon which may lead to synovitis, intrasubstance tearing and tendinosis4. ‘Recent literature has reported a higher prevalence of PTTD in women than in men, but with no explanation for this discrepancy’5.
It is suggested that there are numerous underlying causative factors such as: excessive pronation, trauma, anatomical anomalies (eg. leg length discrepancy), inflammatory joint diseases, acute evulsion, iatrogenic events to name a few.
Many commentators state that PTTD is an overuse condition as the symptoms usually occur after activities that involve stress on the tendon, such as running, walking, hiking or climbing stairs.
The condition has often been categorised as ‘adult acquired flatfoot’ and research concludes that PTTD results in loss of medial arch structure and abduction of the forefoot, resulting in a change of gait4, accompanied by ensuing upper structure issues.
PTTD is categorised as having 3 stages of progression, the duration and severity can move rapidly from acute phase to subacute phase and ultimately chronic. The symptoms of PTTD can include pain and swelling. As PTTD advances, eversion of the calcaneus occurs and the arch often flattens, shifting pain to the lateral aspect of the foot (below the ankle). As the tendon deteriorates arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
A recent study of PTTD Phase 2 patients suggest that non-surgical treatments to consider include reducing Posterior Tendon activity using arch supports/foot orthotics4 and inverting the rearfoot using an orthotic device with an Increased rearfoot varus angle. Inverting the entire orthotic device using an ‘inversion ramp’ can significantly reduce strain on the tibialis tendon.
Inversion Ramp to Invert Orthotic Device
ICB Full Length orthotic fitted with inversion ramp.
The ICB ramps are available in 4°,6°,8° and are 32cm in length.
Inversion ramp on full length orthotic.
Conservative Treatments • Immobilisation: short-leg cast or ‘moon boot’ to allow the tendon to recover.
• Ultrasound therapy and exercises may help rehabilitate the tendon and reduce inflammation.
• Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) to reduce the pain and inflammation.
• Foot Orthotic Devices: to reduce calcaneal eversion/pronation are effective in stages 1-3. The addition of a medial flange to the dorsal arch of the orthotic can provide extra support to the navicular.
Medial Flange to control Navicular
Medial Flange on Orthotic
• Footwear: Shoes that are designed with a flat base that provide good mid foot control and heel cup support can reduce arch collapse. In cases of PTTD that have progressed substantially or have failed to improve with non-surgical intervention, surgery may be required.
References:
1. Merriman’s Assessment of the Lower Limb (2008), 3rd Edition. Churchill Livingstone. p264 2. Plattner PF (1989) Tendon problems of the foot and ankle. Postgraduate Medicine 86(3):155-170 3. Wassef S., Mikhail M., (2008) Ankle, tibilais posterior tendon injuries. Available at: http:// emedi-cine.medscape.com/article/ 386322-overview 4. S.I. Ringleb, S.J. Kavros, B.R. Kotajarvi, D.K. Han-sen, H.B. Kitaoka, K.R. Kaufman Changes in gait associated with acute stage II posterior tibial tendon dys-function Gait & Posture 25 (2007) 555–564 Biomechanics Laboratory, Division of Orthopedic Research, Mayo Clinic College of Medicine. 5. Gehrig Laura MD, Posterior Tibial Tendon Dysfunction: More Prevalent in Women, AAOS Now, Issue: March 2009
A Dorsiflexed 1st Ray (Metatarsal) also known as metatarsus Primus describes a deformity in which the 1st Ray /Metatarsal lies in a dorsiflex position relative to the lesser metatarsals.
The first ray is made up from the first metatarsal and the medial cuneiform. The ray facilitates movement in all three planes however predominantly produces the frontal and sagittal plane movements of dorsiflexion coupled with inversion and plantarflexion with eversion. This is due to its axis being 45° to both of these planes.
The biomechanics of this condition and the compensatory mechanisms and the resultant limitations need to be considered to understand both the function issues and the possible treatment that will need to be proposed for this condition.
The first ray (metatarsal) normally sits parallel to the plane of the lesser rays with equal amounts of dorsiflexion and plantarflexion usually 5mm up and 5mm down to allow the required plantarflexion to enable 65° to 75 °of MPJ dorsiflexion during the propulsive phase.
A Dorsiflexed 1st Ray is an osseus deformity where the lesser metatarsals sits lower to the bisection of the 1st Metatarsal when the foot is in the STJN position.
The condition may be congenital or acquired and is often referred to as ‘metatarsus primus elevatus’ or simply the prime metatarsal is elevated in reference to the lesser.
It should not be confused with Forefoot Supinatus as once the foot is placed in STJN the shaft can, with a supinatus, be plantarflexed. However, we should understand that the dorsiflexed 1st can be both fixed and or mobile in nature.
Because the 1st metatarsal is dorsiflexed it encourages the foot to collapse medially inhibiting the phalange from propelling over the 1st MTPJ, jamming occurs and a reduction in the ROM of the joint may be experienced.
The result of this jamming will be a stiffening of the joint and often the patient will develop an adductory twist in gait to reduce the load on the 1stMTPJ, as this occurs callosity will develop on the medial aspect of the hallux.
The distal phalanx of the hallux can also be forced into dorsiflexion as a toe off compensation, causing a hole to wear on top of the shoe and thickening of the nail from the constant trauma on the dorsal toe.
Clinical assessment of Metatarsal Phalangea Elevatus ( MPE) involves the evaluation of the sagittal plane position of the joint. The patient is evaluated in a non-weight bearing supine position with the subtalar joint in its neutral position (use the ICB AAM method) for Neutral.
As previously stated Metatarsus primus elevatus can be described as being congenital or acquired and can be further classified as a rigid, semi rigid, mobile or hypermobile deformity. A normal range of motion usually indicates a congenital deformity whilst an acquired.
MPE is characterised by an abnormal range of motion. This may be due to tibialis anterior contracture or associated with a forefoot supinatus.
The main issue is that the elevated metatarsal encour-ages the foot to function similar to a forefoot varus and excessive pronation is a key element as the foot collapses medially to allow normal ground contact in the toe off phase. Treatment will be a Morton’s ramp extension.
The purpose of the treatment is to allow a more normal ‘toe off’ to occur in the gait cycle by filling the gap under the 1st MTPJ whilst supporting the proximal hallux and thereby allowing earlier loading to occur.
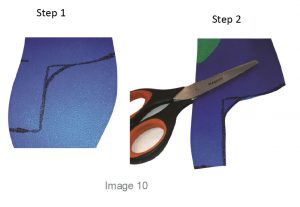
To create the Mortons ramp to lift the proximal hallux this can be achieved by using a ICB 4° Forefoot addition (acts like a Morton’s ramp Image 9) to support the hallux and allow it to propel over the 1st metatarsal joint during toe off stage of gait.
A Full Length orthotic can also be used to create a Morton’s extension, use the forefoot addition to provide the required lift. See image 10 add the addition and mould to the foot in Neutral. First mark out the Morton’s extension ramp shape , cut and use a hand grinder to smooth the distal edges.
Orthotic therapy is not an exact science, so be prepared to adjust the orthotic for the patient by adding or subtracting as needed.
General REFERENCES
1. Merriman, L.M. and Tollafield, D.R. (1995) Assessment of the Lower Limb. Churchill Livingstone, Singapore Figure 2: Evaluation of first ray position(Merriman and Tollafield, 1995)
2. Root M L, Orien W P, Weed J H., 1977 Normal and Abnormal Function of the Foot. Clinical Biomechanics Vol 2, Los Angeles
3.Merriman’s assessment of the Lower Limb 3rd Ed. Churchill Livingstone
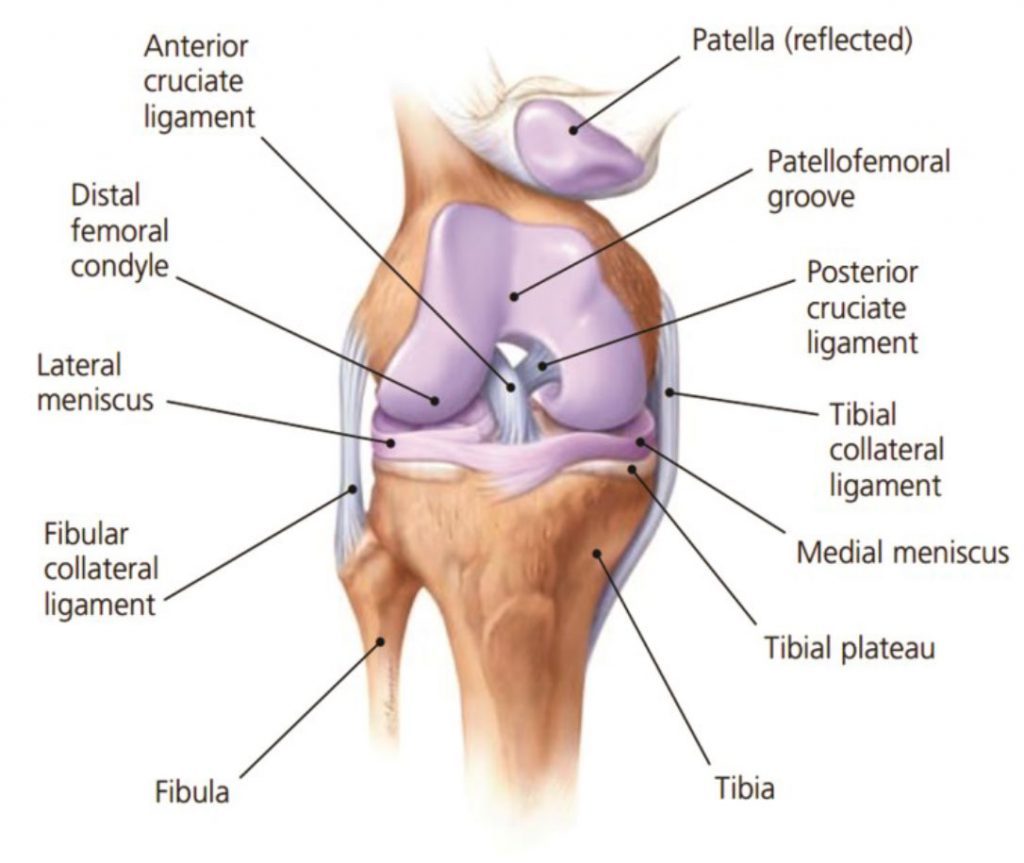
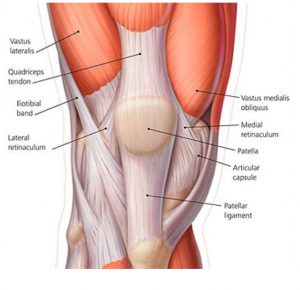
The knee joint is the largest joint in the human body consisting of two articulations: one between the femur and tibia, and one between the femur and patella. It is commonly described as a ‘hinge joint’, being a combination of a hinge and pivot-joint, which permits flexion and extension as well as a slight internal and external rotation.
The knee joint consists of an articulation between four bones: the femur, tibia, fibula and patella, and comprises of four compartments. These are the medial and lateral tibiofemoral compartments, the patellofemoral compartment and the superior tibiofibular joint. The components of each of these compartments can suffer from repetitive strain, injury or disease.
There are many reasons for experiencing knee pain such as, sprained ligaments, meniscus (cartilage) tears, tendonitis, and excessive supination and excessive pronation. The knee is a complex joint, and it can experience pain due to an exaggerated Q angle of the upper leg, for example.
Some of the conditions that can affect the anterior knee compartment are conditions such as :
Patellofemoral pain syndrome
Chondromalacia Patella
Osgood-Schlatter’s disease
Sinding Larsen Johansson syndrome
Knee bursitis/Hoffa’s disease
Generally in this article we will be dealing with non-trauma induced pain or biomechanically induced pain which is often described as idiopathic in nature.
Often when the subject is discussed terms such as ‘Retro Patella pain’, ‘Patella Femoral Dysfunction’, ‘Medial Compartment Syndrome’, ‘Chondromalacia Patella’ or ‘Iliotibial Band Friction Syndrome’ – these conditions are descriptions of knee pain (or pain centres) and do not indicate causative factor/s contributing to the experience of the pain.
Generally pain can be experienced Medial, Lateral or Anterior aspects and it is recommended that the Symptomatic treatment approach is adopted which, treats the pain and then progressively treats the underlying causative factors.
Understanding the dynamics of the knee joint is important in understanding why certain foot mechanic issues can impact upon the knee compartment. The knee is one of the most important joints in our body, playing an essential role in movement related to carrying the body weight horizontally (in running and walking) and in a vertical direction (jumping and absorbing ground reaction impact). The ligaments surrounding the knee joint offer stability by limiting medial and lateral movements, and together with several menisci and bursae, protect the articular capsule.
There is an allowance in the knee joint for a small amount of medial and lateral movement of between 3°-5°. Movement in excess of this puts the patient at risk of experiencing medial collateral ligament and lateral collateral ligament damage.
Both excess pronation and excess supination can have a deleterious effect on the medial and lateral collateral ligaments as outlined by Michaud 1 in which he states that for every 1˚ of pronation and or supination, the tibia internally or externally rotates 1˚, which in turn impacts on the knee joint, as it bears the stress generated by the tibial rotation.
When both excessive internal and excessive external rotation are experienced together excessive movement of the patella ligament occurs and pain can be experienced anteriorly.
Tiberio(2) notes that malalignment factors such as, excessive rotation of the lower leg which accompanies subtalar joint pronation has been cited as a major contributor to patellofemoral dysfunction.
There appears to be a direct link to knee pain from foot mechanics issues and therefore identifying and treating basic lower limb biomechanics appears to have a beneficial affect for patients.
Controlling both pronation and addressing any issues with forefoot will be a determining factor in addressing anterior knee pain.
The medial collateral ligament (MCL) connects the femur to the tibia, whilst the lateral collateral ligament (LCL) connects the femur to the fibula and both work to stabilise the knee by bracing and protecting the sideways movement.
The lateral collateral ligament is placed under stress by lateral biomechanical factors such as supination, internal lateral rotation of the tibial shaft and the impact of an untreated forefoot valgus deformity.
Patients that present with a high forefoot valgus FFTVL in excess of 10° will supinate their foot from heel strike to toe off which will stress the lateral knee compartment.
Excessive pronation will cause internal tibial rotation producing stress on the medial collateral ligament.
Idiopathic anterior knee pain however, is often results from a combination of both pronation and supination in which the anterior patella attachment is aggravated by the Lateral to medial movement in the gait cycle.
A Forefoot Valgus less that 10° will allow the patient to heel strike lateral, the ground ‘reaction forces’ are sufficient to propel the foot into pronation at mid stance to toe off due to the lower Forefoot valgus deformity.
The movement at mid stance, in this situation, is rapid and as the supination to pronation movement occurs the patella tendon moves lateral to medial placing additional stress on the tendon.
Stabilising the foundation and reducing excessive movement around the sub talar joint ( STJ) is essential, a reduction in tibial rotation will have beneficial effects on collateral stress at the knee compartment.
A key point in the orthotic therapy to treat knee pain is that the orthotic is correctly fitted and aligned to the bisection of the calcaneus and the alignment of the tibia or tibial varum angle. Failure to adequately address this issue will result in the patient continuing to exhibit the same foundational instability or allow the patient to, in the case of pronation, to ‘collapse the arch onto the orthotic’ due to the poor rearfoot correction.
Patients often ask if sports tape can be used to treat a condition, in place of customised foot orthotics. Sometimes this arises out of financial considerations, and other times because they do not understand the specific roll that a taping procedure plays when treating lower limb biomechanical dysfunction.
Practitioners can incorporate taping therapy into their treatment regimes to help patients who may be unsure of the value of orthotic therapy, and so identify whether orthotic therapy will be of benefit. Sports taping techniques can be incorporated in conjunction with orthotic therapy for a period of time to provide optimum results for the patient.
There are numerous conditions for which a taping procedure can be beneficial such as, Plantar Fasciitis, Osgood Schlatter condition and knee pain (Chrondromalacia Patella syndrome).
Plantar Fasciitis ( heel spur syndrome) is a classic case where the use of a low dye strapping technique is particularly effective as a temporary treatment to ‘mimic’ the realignment and support provided by an orthotic device. ‘Low dye’ taping seeks to control the foot and lift the longitudinal arch at the susentacula tali area, to limit excessive calcaneal eversion. The mechanism used controls the rearfoot, lifts the arch, shortens the foot structure, which in turn reduces the elongation of the plantar fascia and tension at the calcaneal attachment.
This method of treatment is very effective, however, the sport tape must be replaced within 3-4 days, some patients have allergic reactions to the zinc oxide tape. Low dye taping is especially effective for long term foot pain sufferers, such as Severs Disease and patients with Achilles Pain, when used in conjunction with an orthotic device.
Note in figure 1 (below) how the tape is crossed over in a ‘figure of eight’. Watch the video below for the Low Dye Strapping technique.
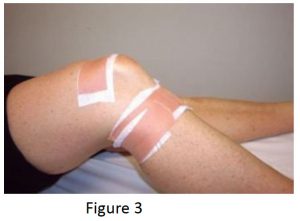
Osgood Schlatter Condition is one which responds very quickly to a combination of orthotics (to treat the excessive pronation) and strapping (to reduce tension on the patella tendon). The complicating issue with Osgood Schlatter is external tibial torsion, which should be treated by a practitioner who uses ‘gait plate’ orthotic therapy to correct the torsion. Growth spurts combined with excess pronation, a highly active child and external tibial torsion are all contributing factors.
Strapping may be used exclusively to treat to Osgood Schlatter (see fig. 2 ). However the condition and associated pain often appears to ‘flare up’ and so controlling the patients’ biomechanics is essential for effective treatment.
Medial knee pain due to excessive pronation can be assisted using orthotic therapy and the McConnell strapping techniques to stabilise the patella. Internal tibial rotation is associated with excessive pronation, resulting in medial displacement of the patello-femoral path and encouraging lateral displacement of the patella (knee cap). See Fig 3 below This is a common problem and elicits pain and around the medial aspect of the patella, especially with excess loading activities such as running.
Internal tibial rotation is also responsible for creating medial collateral strain of the ligamentous structures that wrap around the medial aspect of the knee and lower leg (Cosgarea, 2002).
Excessive pronation causes excessive strain to the medial co-lateral ligament. As a factor of this condition the VMOs weaken and the ITBs tighten, causing external rotation of the femur as a compensation. The patella begins to track on the lateral aspect of the femoral condyle, crepitation and grating feeling is experienced on flexion to extension.
As mentioned strapping using the McConnell technique and strengthening the VMOs is a good treatment regime, however, it will NOT correct the cause of the problem, only assist in pain relief.
Anecdotal studies have supported that in clinical practice, patellar tape provides a useful treatment technique, clinical and research evidence supports relief of pain associated with PFPS (patella femoral pain syndrome)1 The condition and pain will generally recur constantly until the knee has degenerated or become OA (osteoarthritic) – at which time surgical intervention may be needed.
A basic requirement to reduce rotational stress on the knee is control and correction of the STJ (Subtalar Joint) and MTJ (Midtarsal Joint) pronation and this can be achieved with an orthotic device that corrects rearfoot pronation.
The most effective biomechanical treatment for medial knee pain, involves the following 3 steps:
1. McConnell Technique – to control lateral/medial patella displacement.
2. Low Dye Strapping – to mimic orthotic treatment. However, low dye is only a temporary treatment.
3. Orthotics to stabilise the structure and limit excess pronation. The orthotics should be moulded to the patient’s NCSP (Neutral Calcaneal Stance Position) Otherwise described as Ideal position.
This action will control STJ and MTJ pronation – making it more effective in producing long term results for the patient.
REFERENCES :
1. Patellar taping: is clinical success supported by scientific evidence K. Crossley*, S. M. Cowan*, K. L. Bennell*, J. McConnell. Manual Therapy (2000) 5(3), 142-150
COSGAREA, A.J., BROWNE, J.A., KIM, T.K. & MCFARLANE, E.G. (2002) Evaluation and Management of the Unstable Pa-tella, The Physician and Sports Medicine, 30, 10
One of the most profound changes to affect the study of foot function was the theory proposed by Root etal (Root 1964, Root et al 1971) which outlined the concept of a measurable neutral position about which the foot was supposed to function.1
There has been much conjecture about the relevance of Neutral Calcaneal Stance position (NCSP), other-wise described as a patients unique Ideal position. However, still today the ‘Root Theory’ has stood the test of time albeit with alternate theories and modifications to ensure that the process works in a clinical setting.
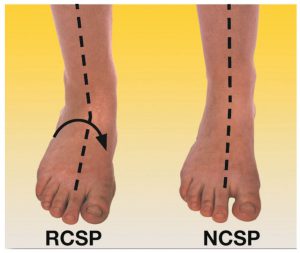
The Foot Posture Index (FPI) 2 is useful in establishing several methodology’s to manipulate the weight bearing foot into a posture that can be considered functionally neutral and quantify the frontal plane position of the foot.3
For clinicians the challenge is to find a fast, effective method of establishing the patients position in which, they are neither excessively pronated or excessively supinated otherwise defined as NCSP or Ideal as opposed to a resting Calcaneal Stance position RCSP. Using of the FPI in a clinical setting could be quite cumbersome as the 6 steps need to be correlated with each other and the time taken could be excessive and highly inefficient.
Most practitioners using orthotic therapy around the world have de-faulted to the Talo navicular method which, at times, made finding congruency difficult due to a lateral osseous exostosis on the talar head often being present Equal ness or congruency is not instance easy to establish.
Therefore a method which can use the FPI and additional method combining together to overcome any anatomical variances such as the ICB Anterior Line Method (ICBAAM) is of particular benefit.
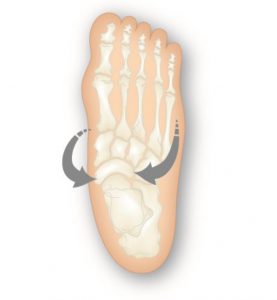
The ICB AAM uses the Talo Navicular reference points aligning the tibia with the 2nd MTPJ by drawing an anterior line.
The Talo Navicular method uses talar head congruency to establish the neutral position.
FIG 1
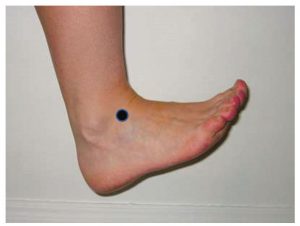
The TN Reference points can be established by placing the foot in a dorsiflexed position4
It may be useful in some cases to move the foot into inversion and eversion while palpating for the talar head This way both eversion and inversion can be clearly identified.
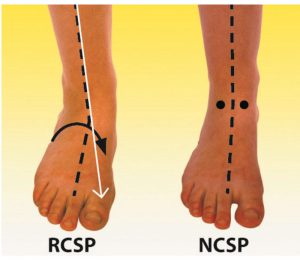
In the resting position the Anterior line will deviate medially indicating that pronation is evident and Laterally if the foot is supinating.
TN reference points are exposed when the foot is dorsiflexed with the heel on the ground.
At rest the tibial varum alignment aligns with the 1stMTPJ on a excessively pronated foot.
The Rearfoot position can also assist in establishing neutral in conjunction with ICB AAM.
There is a direct correlation between rearfoot alignment and anterior alignment position.
When finding the tibial varum angle the practitioner is conceptualising where the Tibia sits within the soft tissue and the same process is undertaken when bisecting the calcaneus.
The ICB Anterior Alignment Method is especially useful when moulding and fitting orthotics as it provides reference points that can be clearly identified when wearing shoes and socks.
Using the ICB Anterior Alignment Method ICB AAM to establish neutral is also useful when taking a foam box casts for custom made orthotics.
NB: every patients neutral may be different, use the established parameters to identify the patients ideal position. and compare with their resting position.
REFERENCES:
1. Merrimans Assessment of the lower Limb 3rd ed p289
2. Development and validation of a novel rating system for scoring standing foot posture: The Foot Posture Index An-thony C. Redmond a,b,*, Jack Crosbie c , Robert A. Ouvrier b 10 May 2005
3. Merrimans Assessment of the lower Limb 3rd ed p290
4. The Orthotic Solution p 29
Michaud T.C., 1993 Foot Orthoses and Other Forms of Conserva-tive Foot Care. Williams and Wilkins, Baltimore, pp.93-105.
Root M L, Orien W P, Weed J H., 1977 Normal and Abnormal Func-tion of the Foot. Clinical Biomechanics Vol 2, Los Angeles
Valmassy, R.L.. Pathomechanics of Lower Extremity Function. Clinical Biomechanics of the Lower Extremity. Mosby, St Louis.