
![]()
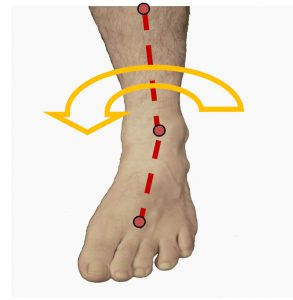
Generally rearfoot supination, inverted position of the calcanaeus relative to subtalar joint neutral or ideal positioning, is not that common and different professions describe it with different terminology eg. Rearfoot valgus is also a term to describe a weight bear-ing/compensated position of the rearfoot. ‘Closed kinetic chain supination consists of calcaneal inversion with talar head abduction and dorsiflexion.’1 it is the collective term for plantarflexion, inversion and adduction of the foot apparatus.2 which is happening around the Sub Talar Joint.


It is correct to say that supination is a fundamental action in the gait cycle and a necessary element, however, in this newsletter we are considering excessive supination or the problematic ‘supinated foot’ structure. Supination of the foot occurs at heel strike to mid stance and then again at toe off and so addressing extended supination and its consequences is important, albeit that the supinated foot occurs in only approximately 8-9% of the population.
Often the supinated foot will present with high arch3 or a more rigid foot structures and upon assessment may exhibit a forefoot valgus deformity.

Patients suffering this biomechanical anomaly will usually wear the lateral aspect of their shoes and experience lateral side joint pain resulting from excessive stress placed on the joints due to the excessive lateral pressure as seen in the Image opposite .
Examining the wear pattern on the patients shoes is a valuable assessment tool as it can indicate the way the body addresses the biomechanical anomaly within the gait cycle, pressure points and wear a tear patterns are often evident.
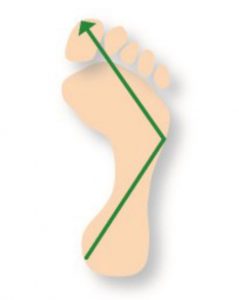
Note: the Lateral wear pattern, in this instance a pattern under the 1st MTPJ indicating a plantarflexed 1st condition.

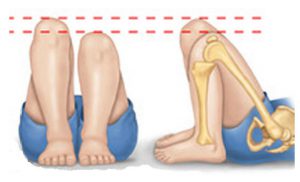
Unilateral supination may be a compensation to structural leg length discrepancy in which the SHORT leg develops a supinated or excessively inverted position to raise the pelvic alignment, in this instance assessing structural leg length is important.
Use a methodology that you are familiar and comfortable with to assist in assessing structural Leg Length.
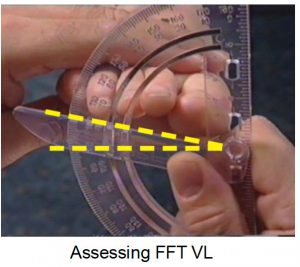
When assessing for ideal or neutral position using the ICB AAM method the foot may need to be everted or moved medially (pronated) to align the 3 reference points of the anterior line.
Anterior view Supinated with ICB AAM line
When a Forefoot Valgus deformity is present the use of a fore-foot wedge addition, will encourage the straightening of the reference lines to enable the practitioner to place the foot into subtalar joint neutral/ideal (STJN).
Most of the ‘off the shelf’ styled or premade orthotics are designed to be anti pronating devices, when treating a supinator these devices will need to be adjusted and modified to suit the supinating patient. Rearfoot supination, if mobile, may be treated with a lateral eversion wedge/ addition, however, mid foot and forefoot inversion (supination) can be treated with forefoot post-ing and lateral eversion ramps.

Often uncompensated (rigid) rearfoot supinators will exhibit a plantar flexed 1st MTPJ as compensation, seeking to enable the 1st MTPJ to make ground contact for toe off phase of gait and will require a 1st MTPJ cut away of deflection to accommodate the plantarflexed 1st.

Supinators will not require rigid or firm EVA styled products, rather mid density or softer materials are best and the orthotic device should be moulded well into the arch.
Generally a curved last shoe is designed for the supinated styled foot. Pronators will require a straight or semi curved last shoe.
Stabilising the forefoot will reduce the inclination to excessively invert or supinate the foot thereby reducing inversion sprain condition.
ICB recommends DUAL Density Sports or Blue mid density styles moulded well into the patients arch.