
![]()
Tibial torsion has been defined as torsion of tibia bone along its longitudinal axis1, which produces a change in alignment of the planes of motion of the proximal and distal articulations, it is a twist in the osseous structure.

This definition draws a distinction between both Tibial Torsion (twist in the bone) and Tibial rotation.
Tibial Rotation occurs when the tibia internally or externally rotates along its axis as a functional outcome of biomechanical forces such as supination and pronation.
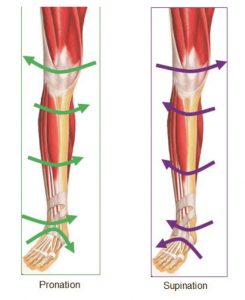
Tibial rotation is the rotation of the entire tibial shaft (bone) which takes place in gait as the foot pronates and supinates. The Tibia can exhibit both torsion and rotation and this makes this subject both interesting and somewhat difficult.
Tibial torsion occurs where the tibia exhibits a twist in the actual bone and is apparent from birth.
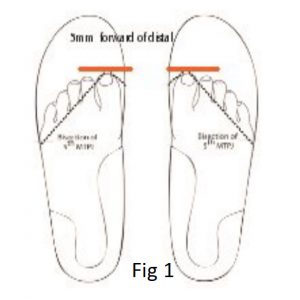
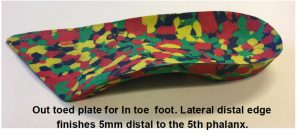
The biomechanical condition can be treated prior to skeletal maturity using foot orthotic devices which work to un torsion the tibia (see Fig 1) .
Once skeletal maturity has occurred, the soft tissue structures are engaged within the body to correct and adjust by tightening and or elongating as the means of correction or repositioning of the foot structure. In both instances knowledge of tibial torsion and tibial rotation will be invaluable to practitioners, in the design and implementation of treatments for their patients.
The broad parameters for identifying Tibial torsion have been outlined by Dr Merton Root 2 and Ronald L. Valmassy DPM3 and others, in which it is stated that torsion of the tibia be undertaken by measurement of the position of the medial and lateral malleoli apexes, (see Fig 2) a technique known as the Malleoli Position. (M.P.) This method imagines a pin bisecting medial and lateral malleoli apexes whilst the knee joint is maintained in the neutral position.

Several tibial torsion measurement techniques have been used or recommended by researchers; radiological methods and arthropometric methods, such as gravity goniometers. The method of measurement generally used in clinical practice is either by eye or by use of a gravity goniometer to measure malleoli positioning. (see Fig 3)
By Eye assessment

Gravity Goniometer
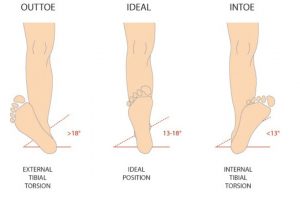
Root and Valmassey reported that the average normal position of the normal malleolar position M.P. was 13° – 18° 2, or slight out toed position.
The malleolar position is determined by observing the bisection of apex of the medial and lateral malleolar whilst the knee joint remained in the neutral position and the patient in the supine position.
Due to the occurrence of displacement of the patella it should be noted that research groups stipulate the position of the knee joint not patella as neutral in the sagittal plane. The positioning of the knee joint was achieved by the using of the knee condyles and lifting in the sagittal plane, ensuring that no lateral or medial deviation is observed.
There are believed to be several causes of the Tibial Torsion condition such as :
a) Acquired: due to injury / trauma such as a broken tibia which is re-positioned and takes on a post-operative internal or external position.
b) Genetics: congenital which is inherited from the mother, father or their genetic lines.
c) Acquired or caused by the environment, especially the uterine environment such as positioning in the womb – the tibia can form in an internal or external torsion position.
When treating in the field of paediatrics it should be noted that Tibial Torsion can effect the gait pattern which, if left untreated may have considerable affect upon the child as it grows to maturity. The outcome may leave the child’s biomechanical structure compromised, leading to other pathologies as the body seeks to compensate for these changes.
Traditionally paediatric biomechanical foot problems were given a low priority, with the result that manageable cases were left untreated and secondary features related to structural pathologies developed. Michaud comments that – ‘Early recognition and management, of actual foot problems in the young would go a long way to the reduction of issues later in life’ 4.
‘Gait plate’ orthotic treatment is a simple and effective method of restoring the lower limb to the ‘normal Malleoli Positioning range of 13° to 18° for children over the age of 6 years.
The gait plate orthotic device is manufactured to provide an extension under the 5th phalange for in-toe or under the hallux for out-toe. In gait the gait plate extension is identified by the proprioception system in the body and the brain instructs the body to reposition the foot in an automated response pattern, gently working on removing the bone torsion in an attempt to reposition to the 13-18° position.
The method is gentle and persuasive and has measurable results , however it appears to be most effective during ‘growth spurts’ in children.
If left untreated the body will naturally attempt to correct by using soft tissues to cosmetically correct the in toed or out toed position. Abnormal foot positioning, i.e. that which is opposed to what is accepted as ‘ideal’ or normal, encourages the body to use soft tissue to en-gage compensatory mechanisms.
Some studies have actually concluded that tight rotators and adductors have a compensatory repositioning function, as in the case of out toe and in toe positioning, relating to tibial torsion. 5,6,7,8, Again it must be stated that this is not strictly the case in every situation, and as such a small number of patients may present with tibial torsion without exhibiting hip compensations. The reasons for a lack of compensatory muscle tightness are unknown. These compensatory mechanisms can move joints in the body outside the normal range of motion and in the pro-cess may lead to so called ‘idiopathic’ soft tissue tight-ness such as Tight Abductors & Adductors or alternatively joint soreness during the compensation process.
References:
1. MULLAJI Arun B, SHARMA Amit K,1 MARAWAR Satyajit V, and KOHLI AF. Tibial Torsion in Non-Arthritic Indian Adults: A Computer Tomography Study of 100 Limbs.
2. ROOT ML, ORIEN WP, WEED JH, HUGHES R, Biomechanical Ex-amination of the Foot The Orthotic Solution I 67 Vol 1. p34, 1971
3. VALMASSY R.L., (1996) Clinical Biomechanics of the Lower Ex-tremeties. p255
4. MICHAUD, T.C (1997): Foot Orthoses and Other Forms of Conserva-tive Foot Care. Sydney: Williams & Wilkins, p168.
5. STAHELI, LT. In-toeing and Out-toeing in Children. Journal Family Practice. May 1983;16(5):1005-11.
6. STAHELI LT, CORBETT M, WYSS C, KING H. Lower Extremity Rota-tional Problems in Children. Normal Values to Guide Management. American Journal Bone Joint Surgery Jan 1985;67(1):39-47.
7.DAVIDS JR, DAVIS RB. Tibial Torsion: Significance and Measure-ment. Gait Posture. Jul 2007;26(2):169-71.