
![]()
Leg length inequality and the pathogenesis or the origin of the condition, is and will always be, a controversial subject. There is not enough space to conduct a debate on the treatment, origin and possible associated compensatory mechanisms that may arise when we examine the topic. Also a wide variance of opinion exists on the significance of structural leg length and the various methods for measurement.
Many texts define minor structural leg length discrepancy as, less than 2 cm of difference. Other studies have suggested that, 40-70% of the population have at least some degree of LLD1, larger differences also appear in .001% (1:1000)of the population. From ICB’s perspective in dealing with Lower Limb Biomechanics, a 2cm structural difference is, rather than being minor, quite a significant amount and should be treated mechanically.

Leg length discrepancy or anisomelia, meaning a difference in length between paired legs, can broadly be categorised into two types:
1. Structural leg length difference, a difference in the long bone measurement of the leg. Its root cause can be illness, hereditary or trauma-related. The etiological factors involved in the causative process can be numerous such as: Idiopathic developmental abnormalities, fracture, trauma to the epiphyseal endplate prior to skeletal maturity, degenerative disorders, Perthes disease, cancer or neoplastic changes and Infections to name a few.
2. Functional differences can be more difficult to identify and treat as the etiological factors can be difficult to diagnose, e.g: body compensation associated with trauma, shortening of soft tissues, joint contractures, ligamentous laxity, axial misalignments, foot biomechanics, such as, unilateral excessive pronation, pelvic rotation and pelvic flare to name a few.
Often structural short leg syndrome is a commonly un-recognised condition that often goes untreated. It can be argued that even small discrepancies of only 4mm, if uncorrected, may over time set off a chain reaction of symptomology throughout the body.
There are 3 types of short leg issues that have been attributed as causative factors: inherited biomechanics, postural habits and or trauma:
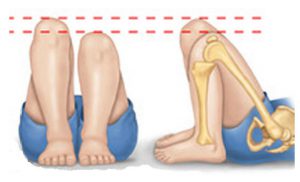
1. Structural Short Leg: when the measurement from the head of the femur to the lateral or medial Malleolus measures shorter on one side than the other.
2. Functional Short Leg: when the measurement from the 2 same reference points are equal on both sides, but there still appears to be a short leg – usually due to a twist in the pelvis.
3. Combination of Structural and Functional Short Leg.
Symptoms
Common symptoms may include:
• Neck and shoulder pain
• Back ache & Hip pain
• Foot pain, Ankle pain, Knee pain.
Muscular, Vascular and Neurological systems may also be affected. Osteoarthritis in the joints, and Scoliosis (including idiopathic’) are classic indicators of a leg length discrepancy and or twist in the pelvis.
Biomechanical Aetiology

Anecdotal observation indicates that 80% of compensations is excessive long leg pronation. If the pelvis does not level as a result of the excessive pronation, the pelvis may twist or drop to one side – causing either a scoliosis or prolapse of the vertebral discs. Unilateral tightness in the gluteal muscles may occur with posterior pelvic tilt and rotation, which in the case of a functional short leg has the effect of rotating the pelvis posteriorly-effectively causing increased rotation of the spine at L1 to L5. A tendency to repeatedly pull (overstretch) the same muscles even though it has been given sufficient time to heal may occur.
A unilateral bunion is often associated with a leg length discrepancy. As the body excessively pronates to provide long leg compensation (to level the pelvis), this predisposes the longer leg to the formation of a HAV or bunion 2. Thus when bilateral HAV is evident and there is unequal Bunion growth, it can be deduced that a longer leg may be evident.
Assessment
Although some Physicians still use measurement methods such as Knee height and tape measure. Current research indicates that newer manual techniques and radiographic analysis are preferred over the old tape measure method.
There are many ways to measure leg length, 2 of the most reliable methods are:
1. CT Scanogram: a radiographic technique that measures the actual length of the tibia and fibula bones. Point of failure in this method could be the inability of the radiologist to match the measurement reference points, however, this is not usually an issue.
2. Supine medial malleoli asymmetry (manual) (Fig : 4): A technique which is becoming more common and certainly more popular is a process that osteopath Gary Fryer at RMIT University Melbourne 20053 known as The Palpation for Supine Medial Malleoli Asymmetry Technique. This method is we believe, quick to perform and has demonstrated both a high intra-examiner and inter-examiner reliability. The trial concluded that Intra-examiner and inter-examiner reliability was almost perfect following subject selection for malleoli asymmetry, suggesting that clinicians can reliably detect medial malleoli asymmetries of greater than approximately 4 mm difference. The patient is placed in the supine position.
The Practitioner balances the hips and pelvis, then marking the inferior aspect of the medial malleolus with a pen. Align the malleoli and rub together to compare the pen line markings, checking for discrepancy between the two lines.

Treatment
In the case of a structural leg length discrepancy, a heel lift alone to the short leg may not provide the solution for the patient, as the long leg will continue to pronate and cause upper body imbalance and compensations. Correction to the longitudinal arch of both feet and their biomechanics by prescribing an orthotic device is essential.
The orthotic device will ensure the correction and realignment of the feet, and the addition of a heel lift on the shorter leg will prevent jamming in the hip of the longer leg, and prevent upper body compensations and resultant pain.
Generally 80-85% of compensatory action will be excessive long leg pronation, other compensations may occur such as : Long leg knee flexion, short leg supination, genu recurvatum or knee hyperextension as a means to adjust the pelvic alignment.
References
1. Woerman AL, Binder-MacLeod SA. Leg length discrepancy assessment: accuracy and precision in five clinical methods of evaluation. J. OrthopSports Phys Ther 1984;5:230-8.
2. Neale’s disorder of the foot 8th edition 2010 p103
3. Gary Fryer 2005 : Factors affecting the intra-examiner and inter-examiner reliability of palpation for supine medial malleoli asymmetry.