

This article will focus on lateral sprain and pain associated with a pes cavus foot structure and a forefoot valgus deformity. Repetitive lateral ankle sprain or lateral knee pain (or even lateral shin splints) is often diagnosed as ‘idiopathic’, closer examination of the biomechanical relevance needs to be pursued. The term ‘idiopathic’ is often used in this area as there seems no reason for the pain occurrence. Pes cavus foot (high arch) structures (Fig. 2) may have a predisposition to lateral ankle sprains and present as a rigid structure and a supinated foot structure.
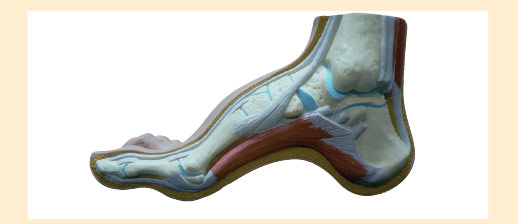
FIG2
This type of structure will usually exhibit a forefoot valgus deformity
meaning that, ‘the plantar plane of the forefoot remains everted relative to the plantar plane of the rearfoot when the subtalar joint is in neutral.’
This deformity will have an impact on the patient in heel strike, midstance and toe-off phases of gait. The patient who exhibits a pes cavus foot structure will often present with a forefoot valgus (FFVL) greater than 10º and also often exhibit a plantar flexed 1st metatarsal
(Boyd & Bogdan, 1993) – encouraging the foot to strike laterally and eliciting pressure on the lateral aspect of the hip joint. If the forefoot valgus deformity is greater than 10º, the foot will often continue to supinate through the cycle, having a ‘jarring’ effect on the upper structure, putting additional strain on the lateral aspect.

Fig. 3: Use an ICB Protractor to assist in
measurement of Forefoot valgus.
When the foot is supinated it often exerts stress on the peroneals and may cause elongation of the muscles and tendons, thus weakening the retinaculum and lengthening the peroneals, often causing the tendon to sublux off the lateral aspect of the malleolar.
The forefoot valgus deformity (in gait) encourages the foot to invert the foot, propulsion is delayed causing lateral instability and results in tension and tearing of the peroneal muscles, causing inflammation and tenderness, and difficulty walking. Lateral ankle sprains are more common than medial due to the fact that ligaments are weaker on the lateral side.
Hence the lack of lateral stability can be caused by uncompensated or partially compensated rearfoot, a flexible forefoot valgus or osseous forefoot valgus (Boyd & Bogdan, 1993; Hollis et al, 1995; Shapiro et al 1994).
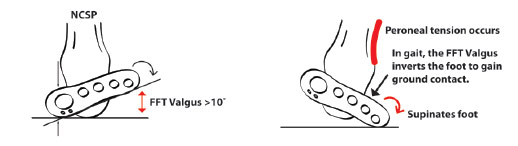
Fig. 4: Effects of Forefoot valgus during gait.
There are also certain biomechanical foot deformities that make some patients more susceptible to inversion sprains, such as, neurological deficits and supinated foot types which exhibit or function with a supinated calcaneus (Valmassy, 1996).
In summary, if a patient presents with lateral hip pain, knee pain, ankle strain or repetitive lateral inversion sprain, always check for a forefoot valgus deformity. If a forefoot valgus if present, add an appropriate size ICB Forefoot Valgus wedge (available in 4° & 6°) to the selected ICB Orthotics using the 3M tape provided. Next, heat mould the ICB Orthotics to the patient’s Neutral Calcaneal Stance Position. Being made from 100% EVA, ICB Orthotics can easily be heated and moulded to suit high arch foot structures.

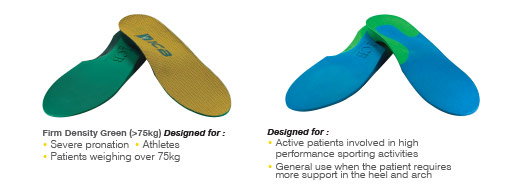
Prescribing ICB Orthotics.
ICB Heat Moulding Orthotics can be prescribed to assist in the treatment of excessive pronation and supination, and resultant biomechanical conditions. With 5 densities, 5 styles & 11 sizes, there is an ICB Orthotic to suit all footwear styles, patient ages and activity levels.

 PRICES START FROM £18.85
PRICES START FROM £18.85
To enable quick and easy orthotic customisation in the clinic setting, ICB Orthotic Additions are also available, including: Forefoot & Rearfoot wedges, Heel Lifts, Metatarsal domes, medial flanges,
medial arch infills and more.
View the full ICB Orthotic range