
![]()
The topic of Forefoot valgus is an interesting one due to the confusion that often arises as to whether it is an actual Forefoot Valgus or as is often the case a misdiagnosed Plantarflexed 1st and vice versa.
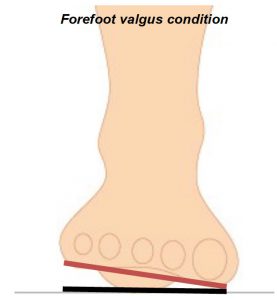
A forefoot Valgus deformity can be defined as ‘When the plantar plane of the forefoot remains everted relative to the plantar plane of the rearfoot when the sub talar joint is in the neutral (STJN) or patients ideal position.
Conjecture often arises as to whether the condition is solely genetic or acquired.
Forefoot Valgus has been described as a position in which a constant structural eversion of the forefoot exists and presents as the most common structural or positional deformity in the forefoot.
It is an everted position of the forefoot relative to the rearfoot at the level of the midtarsal joint. Inversion of the lateral column of the foot must occur to allow the forefoot to move to a pronated position during the midstance and then resupinate during the propulsive phases of gait.
There are generally two forms of forefoot valgus referred to in most texts:
1. Flexible forefoot valgus – This exists where there is sufficient flexibility in the midtarsal joint to allow the lateral column of the foot to reach the supportive surface during the stance phase of gait. The heel may function perpendicularly, but the amount of compensation that occurs leads to an unstable gait with late pronation through midstance into propulsion.
2. Rigid forefoot valgus – Where the range of motion in the midtarsal joint is not enough to allow the lateral column of the foot to touch the ground, rearfoot supination compensation is required to allow lateral strike and gait progression. This is a rarely seen condition clinically.
Generally the following issues are observed in Forefoot Valgus conditions or anomalies.
In the case of acquired it may be the result of surgery or as a compensation due to other issues which present and mechanically can present as rigid or functional.
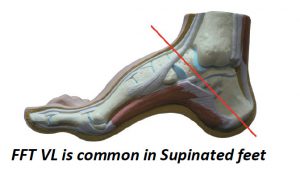
Forefoot Valgus feet usually experience Excessive supination at the STJ accompanied by external rotation of the leg with resultant lateral instability of the knee, ankle and Sub Talar Joint. Forefoot Valgus feet will often present as a pes cavus structure exhibiting a loss of shock absorption mechanisms in lower limb with induced lower-back, hip, knee and shin pathologies.
The 1st MTPJ unlocks when supinated, with resultant forefoot hypermobility. A common com pensation is that a Plantarflexed 1st will present with the forefoot valgus to allow the 1st MTPJ to plantarflex to gain ground contact and thereby enabling gait positioning and toe off to take place.
Another common condition that may accompany the Forefoot valgus is a Tailor’s bunion and other conditions such as Plantar digital neuritis. Lateral Plantar fasciitis pain and Medial Sesamoiditis can occur together with Compensatory calcaneal (Sub Talar Joint ) pronation leading to Haglund’s deformity.
However when assessing often the forefoot valgus is misdiagnosed as a Plantarflexed 1st Metatarsal whereas both conditions can occur at times, in combination.

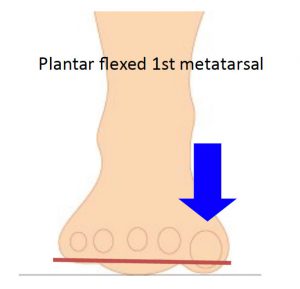
A plantar flexed 1st occurs when the 1st Metatarsal joint sits plantarflexed to the lesser metatarsals, when the subtalar joint is in neutral. It can be either mobile of fixed (osseous).
Forefoot Valgus assessment
When assessing Forefoot Valgus commence by establishing the neutral or patients ideal position in supine Use the Anterior alignment to identify the neutral position.
Use the Left hand on the patients Left foot to ‘feel’ for Talo navicular congruity, whilst observing the Anterior Alignment position using ICB AAM technique.
Dorsiflex the 4th and 5th metatarsal Phalengeal joint to resistance whilst maintaining 10°of plantarflexion of the foot.
This is the most crucial part as, in assessment, one should not dorsiflex the foot past the point of resistance as this can ‘manufacture’ or create a forefoot valgus where none.exists
Observe the Anterior alignment ensuring that the 2nd metatarsal head is aligned with the Bisection point of the Talonavicular reference points and the Tibial crest on the lower 1/3 of the leg.
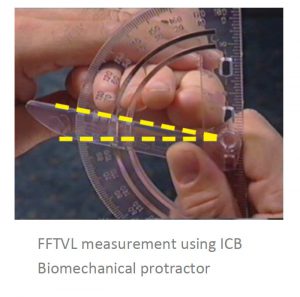
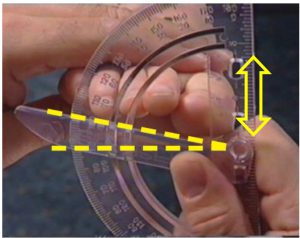
Compare rearfoot plane and forefoot plane and measure the amount of posting that needs to be applied to the orthotic using an ICB Biomechanical protractor. (see below) As a general rule, post only 1/2 the measured amount, or use the posting formula ouline in The Orthotic Solution book page 161 and 201.
To check for Plantarflexed 1st once you have dorsiflexed to resistance, take hold of the lesser metatarsals and maintain that position whilst
completing the assessment for plantarflexed 1st i.e. palpate the 1st MTPJ 5mm dorsiflexed to 5mm Plantarflexed whilst holding the lesser metatarsals in the Valgus position
See also: The Orthotic Solution book Pages 34, 77, 160, 201
SAVE 10% OFF ICB PRODUCTS WITH DISCOUNT CODE: 02ICB10 Offer online only!