
![]()
Back pain is a complex one as it can be categorised into a variety of locations Upper, Middle, and Low Back Pain, and can range in intensity from mild to severe (chronic). Sciatica for instance, can cause pain in the lower back and the legs, where-as low back strain can affect L1 –L5 region of the spine. Excessive pronation can also cause lower lumbar pain due to its affect of rotating the pelvis anteriorly. A short video on Back pain is below.

Treating this pain requires that we determine wherever possible, the origin of the disorder whether from the muscles, nerves, bones, joints or other structures in the spine.
It is reported that low back pain causes 40% of missed days of work in the United States1, and is reputed to be the single leading cause of disability worldwide2.
The spine is a complex interconnecting network of nerves, joints, muscles, tendons and ligaments, all of which are capable of producing pain. Therefore in this newsletter we just want to focus on basic back pain associated with structural leg length abnormality and how to treat these problems by incorporating orthotics and other modalities.
Leg length can, we believe, be categorised into two basic areas:
1. Structural – a difference in the long bone measurement of the leg and,
2. Functional – arising from a variety of causes which affect the biomechanics of the body.
When a patient presents with back pain a determination of the underlying factors needs to be undertaken. Always start with the basics, and complete a full biomechanical assessment, which includes long bone measurement and a comparison of the amount of pronation/eversion and supination/ inversion at the foundation. The first thing to look for is whether the patient is presenting with bilateral or unilateral pronation. If it is UNILATERAL, establish if the patient has:
a. suffered a trauma in which one plantar fascia may have ruptured or elongated and consequently, created a functional short leg or if there is idiopathic ulilateral excessive pronation or supination present.
b. assess if tibial torsion with hip compensation is present : such as tight psoas which will rotate the pelvis anteriorly, or tight piriformis ITB’s and Gluteals, as a compensation for internal tibial torsion to correct the pigeon toed position. Both these compensations could either, rotate the pelvis (anterior) forward or (posterior) backward creating functional leg length problems in the gait cycle.
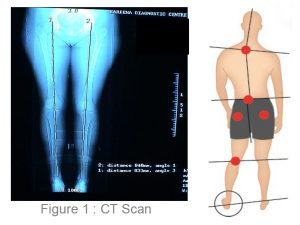
If the patient has a long leg compensation in which the long leg drops down or pronates to level the pelvis, establish the structural length and this can be verified using a CT scanogram (see Figure 1) for leg length or the normal x-ray film to check the leg length.
The longer leg will be predisposed to hip joint wear and tear. Therefore if a patient is asymmetrical, inform them about the consequences of not treating the condition. Some practitioners say the body will compensate for the difference so why bother with a heel lift to raise and level the pelvis? However, even everyday objects that are asymmetrical such as tables and chairs become unstable over time, how much more our bodies?
It has been said that 3-4mm can upset the biomechanical structures of the body.
If the patient is suffering from hip compensations they will need to be either referred to the appropriate Allied Health Practitioner for stretching and strengthening exercises to correct the anomaly. At the same time prescribe orthotics to realign and correct the biomechanics. A combination of orthotic therapy and muscle stretching and strengthening will give the best treatment results.
If there is no apparent structural leg length the use of orthotics to realign the foundation will be required and a combination of other modalities will be needed to address both skeletal and soft tissue imbalances and compensations.
When the patient presents with a structural deformity either due to a recent trauma or a long term biomechanical related anomaly, the use of a heel lift or raise on the structural short leg will be required.

It is recommend that the practitioner applies ½ the leg length discrepancy measurement, in the heel lift. Then this amount can be gradually increased, this will limit initial discomfort and quicken patient compliance. In the case of treating a short leg due to trauma/ accident injury the entire amount can be applied, within the first 6 months, as long as the rehabilitation has ceased and the body has not started to use soft tissues to compensate for the leg length deficiency. Contraindication in these instances would be any fusing of the spine as this may cause the patient to be in more pain.
If you are prescribing orthotics and have NOT MEASURED structural leg length, the orthotic will invariably remove the any normal body compensation of the ‘long leg pronation’. If excessive long leg excessive pronation compensation is removed it will create a jamming in the long leg acetabulum at the hip, create problems with the SI joint and contribute to the development of a scoliosis, as stated in Blake & Ferguson, 1992.
Placing a heel lift in the shoe of the short leg without using orthotic devices is not recommended, as this will create a leg length problem on the raised leg side, because the longer structural leg will continue to pronate due to ligament laxity. The use of one orthotic is never recommended as the foundation needs to be balanced, and the necessary biomechanical corrective additions attached to the orthotic.
Where back pain and SI joint pain is concerned it is recommend that leg length discrepancy is assessed and treated.
Treatment
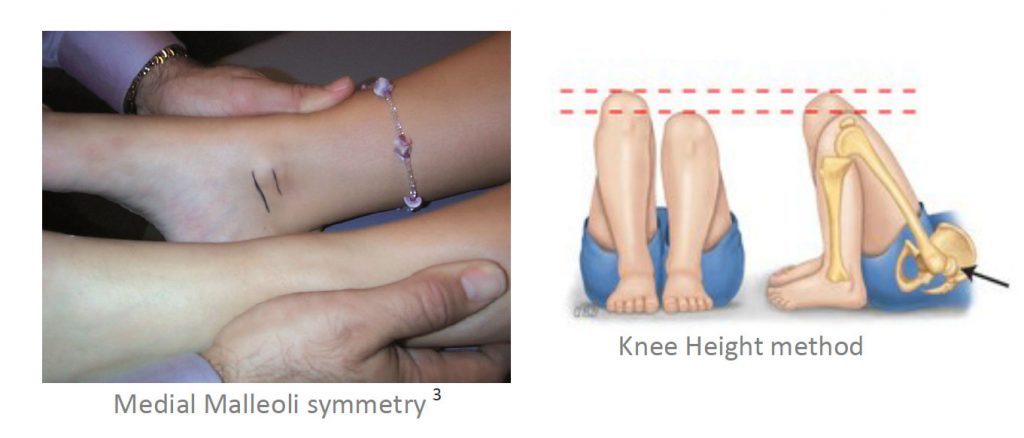
Measure and confirm structural or functional leg length discrepancy. Use a method you are comfortable with.
• Orthotics to treat ‘long leg pronation’, together with a heel raise being added for the short leg.
• Raise the short leg in stages – if the discrepancy is a large, start with half the amount of measured discrepancy.
• Often a multi-disciplinary approach such as adjustments to ‘free’ the pelvis, stretching tight muscles is beneficial. Check the head of femur is sitting correctly in the acetabulum, in combination with orthotic therapy will deliver the best results for the patient.
REFERENCES: